AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2578-8949/015
*Corresponding Author: Marco Wesley, Department of Dermatology, Amsterdam, Netherlands.
Citation: Marco Wesley, Garrett Kenneth, Isaiah Connor, Ryan William. Infectious Dermatoses are Common in Primary Health Care Setting in Côte d’Ivoire. J .Dermatology and Dermatitis. Doi: 10.31579/2578-8949/015
Copyright: © 2017 Marco Wesley. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 December 2017 | Accepted: 26 December 2017 | Published: 30 December 2017
Keywords: infectious dermatoses; community health; primary health care; socioeconomic conditions
Background: Infectious dermatoses are common in many countries in Africa. These skin conditions mostly caused by bacterial, fungal, viral, and parasitic agents are frequent in primary health care setting. These are favored by poverty that deprives individual of the freedom to satisfy basic needs and rights: this includes freedom to enjoy clean water or sanitary facilities, and good accommodations or remedies for illnesses.
Objective: This study was conducted to show the frequency of infectious dermatoses in a primary health center in Côte d’Ivoire.
Methods: It was retrospective and descriptive study conducted in the community health care center in Yopougon Attié from 2006 to 2010.
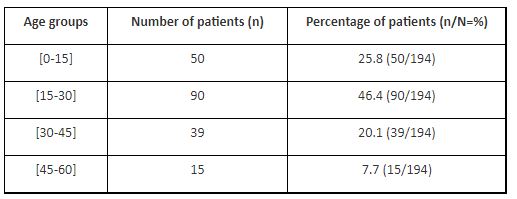
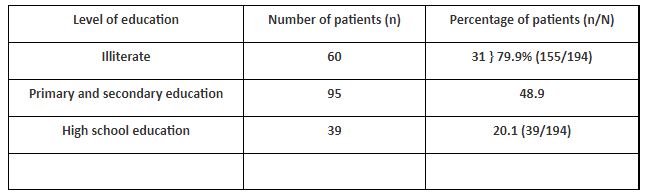
Results: About 3.392 patients out of 22.609 (15% of cases) were admitted for dermatoses during a period of 5 years. Only 203 patients got accurate diagnosis for dermatoses. Sixty three patients were males (32.7%) and 135 were females (67.5%). The sex ratio was 2.08 in favor to females. Patients’ age ranged from 6 months to 59 years with average age of 27 years ±2.2. Patients from age group between 15 and 29 years were the most concerned (46.4%), followed by the age group under 14 years (25.8%). Illiterate or primary and secondary education patients (79.9%) were mostly observed. Adverse socio-cultural practices were performed in 56.7% of cases. We observed infectious dermatoses in 92.12% of cases (194/203) infections due to bacterial agents were most observed in 42.6% of cases, followed by viral agents in 31.95% of cases. We found HIV positive patients in 5.7% of cases.
Conclusion: Infectious dermatoses are common in primary health care setting in Côte d-Ivoire and can be treated by any physician. But, a dermatological training is needed to improve primary health care practitioners’ dermatological skills for clear diagnosis and appropriate treatment in order to reduce their incidence and prescription costs.
Skin diseases pose a significant public health problem in many countries in Africa and they are mainly a result of common conditions that are due to preventable infections and infestations. In Tanzania, infectious dermatoses account for up to 85% of skin conditions and 71% of cases in Ethiopia [1,2]. These infectious dermatoses are mostly caused by fungal, parasite agents and sometimes bacterial and viral agents [3]. In Côte d’Ivoire, infectious dermatoses remain frequent issues in primary health care setting, where there are no dermatologists. We conducted this study in a community health care center in order to appreciate the frequency of infectious dermatoses at a primary health care level in order to initiate a strategy for prevention.
It was retrospective and descriptive study based on patients’ medical records seen in consultation office during the time period of 5 years (from 2006 to 2010). The study was conducted in the community health care center in Yopougon Attié, a neighborhood of Abidjan the economic capital of Côte d’Ivoire. All patients presented a dermatosis with an accurate diagnosis were included. Patients were recruited whatever their sex and ages. We reviewed the clinical records of all patients using a questionnaire including demographic details (sex, age, level of education, adverse socio-cultural practices), clinical dermatological finding of skin infections as well the type of cutaneous infections. The HIV status was checked as well as water availability and bathing.
Data recording were done using Word 2007 software and Excel under windows XP For graphic drawing. For data analysis, we used EPI info version 6.04.
In total, about 3.392 patients out of 22.609 (15% of cases) were admitted for dermatoses during the study period (3 years). But, only 203 patients got accurate diagnosis for dermatoses. These 203 cases of dermatoses for which diagnosis was made based on clinical manifestations represented about 0.90% of cases (203/22609). Sixty three patients were males (32.7%) and 135 of them were females (67.5%). The sex ratio was 2.08 in favor to females. The age of our patients ranged from 6 months to 59 years with average age of 27 years ±2.2. Patients from age group between 15 and 29 years were the most concerned (46.4%), followed by the age group under 14 years (25.8%) (Table 1). Most of our patients (79.9%) were illiterates or had primary and secondary education level (Table 2). The majority of our patients took their baths twice and more per day with clothes change in 97.9% of cases. Adverse socio-cultural practices were performed in 56.7% of cases; there were mostly scarification and traditional mixtures for skin care. Conversely, 43.3% cases of our patients did not perform these practices. Most of the patients in our series got adequate clean water supplies.
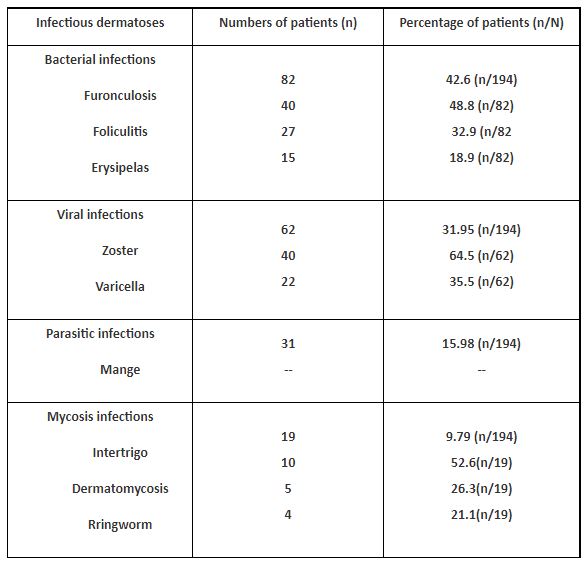
We observed infectious dermatoses in 92.12% of cases (194/203) and only 04.43 cases of non-infectious dermatoses (09/203). Infections due to bacterial agents were mostly observed in 42.6% of cases, followed by viral agents’ infections in 31.95% of cases (Table 3). We found HIV positive patients in 5.7% of cases. In our series, 150 patients (73.9% of cases) were healed at the primary health care setting conversely 53 patients (26.1% of cases) were referred to the dermatologist for treatment.
In poor countries, although skin diseases are common, the majority are caused by a small group of conditions, many of which are infectious [4]. The prevalence of infectious diseases found in our study was 92.12%. This rate was above the 72.3% reported in Nigeria by Kalu [5]. The rates found in these studies could be a reflection of the defective environment health conditions such as lack of sanitary facilities, dirty environment and promiscuity with overcrowded household. As it was stated that high prevalence of infectious dermatoses is an index of socioeconomic development level [6]. But, other studies reported lower rates of infectious dermatoses. In the study of Tay [7], infectious dermatoses were mostly observed in 23.4% of cases after eczema or dermatitis in 33.1% of cases. In study conducted in Ghana, the five common skin conditions seen were infections, dermatitis, pruritus, autoimmune diseases and acne. The high frequency observed in their study was attributed to hot, humid climate as well as to adverse socioeconomic conditions [8]. In our study, the majority of our patients have done adverse socio-cultural practices in 56.7% of cases, which could also favor skin infections. These practices are mostly performed in septic conditions.
We observed more infectious dermatoses in males than in females. This observation could be explained by the fact that female care more about the physical appearance, therefore the personal hygiene. This finding corroborates with those found in the literature [5].
As observed in previous study, we found the four etiologic classes of infectious dermatoses including: bacterial, viral, parasitic, and fungal infections in 42.6%, 31.95%, 15.98% and 9.79% of cases respectively. The preponderance of bacterial dermatoses is linked to poor individual hygiene and dirty environment. This observation could be explained by the fact that the high proportion of our patients belong to age group under 14 years. This category of patients needs parents’ supervision for good bathing.
The high prevalence of viral infections in our series as it was found in literature [5], could be explained by the possible inadequate immunization coverage or the depression of the immune system, as patients were found HIV positive in 5.7% of cases in our series. All these infectious dermatoses are favored by several factors such as: poor sanitary conditions, sharing personal effects and poor access to medical and water supplies. In additions, a factor like overcrowding creates a hot humid environment that predispose to such skin infections by skin contact [3]. It is recognized that poverty deprives individuals of the freedom to satisfy basic needs and rights. This includes freedom to enjoy clean water or sanitary facilities and good accommodations or houses or remedies for illnesses. In this pathway, 12 global public health priorities were advised to be adopted including, to integrate dermatological activities in developing countries into the general health care system at the primary health care level not only at the secondary and tertiary care levels, as outlined at the Alma Ata conference [9,10]. Therefore, a national dermatology training section’s program should be held in Côte d’Ivoire, as it was done in Mali [11], to strengthen dermatological skills and knowledge of doctors or nurses or midwives at primary health care level. In this program initiated in Mali, 400 health care workers were trained for dermatological skills. After a single day training, a marked improvement was seen in term of management and diagnosis of skin diseases in primary health care centers. In fact, between 6% and 24% of the total number of visits to primary health care centers have been reported to be result of skin diseases, as we found in our series (15% of cases) [11]. In addition, in USA, undermatologists treat almost 60% of these skin, hair and nails diseases, and skin disorders are accountered by 20% to 25% of patients seen at the primary health care level [12,13]. All those show the importance of dermatologists or health practitioners with dermatological skills at the primary levels of the health care system in all countries.
Infectious dermatoses are common in primary health care setting in Côte d’Ivoire. Even if they can be treated by any physicians, a minimum of dermatological training sections are needed to enhance physicians’ dermatological knowledge and skills for clear diagnosis. Therefore, they could raise the population awareness, and contribute to infectious dermatoses appropriate treatment and prevention, in order to reduce its incidence and its prescription costs at primary health care level.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.





























































